
Shortness of Breath (Acute Dyspnea)
Shortness of breath, medically termed acute dyspnea, is one of the most common and potentially life-threatening presentations in emergency medicine. It may arise from respiratory, cardiac, metabolic, allergic, neurological, or systemic causes. Because oxygen delivery is essential to every organ system, prompt evaluation and stabilization are critical to prevent rapid deterioration.
Patients often describe difficulty breathing, chest tightness, air hunger, rapid breathing, or inability to take a full breath. Symptoms may develop suddenly or progressively. Associated features such as chest pain, wheezing, cough, fever, leg swelling, fainting, or anxiety provide important diagnostic clues. The severity of distress, ability to speak in full sentences, and use of accessory muscles help determine urgency.
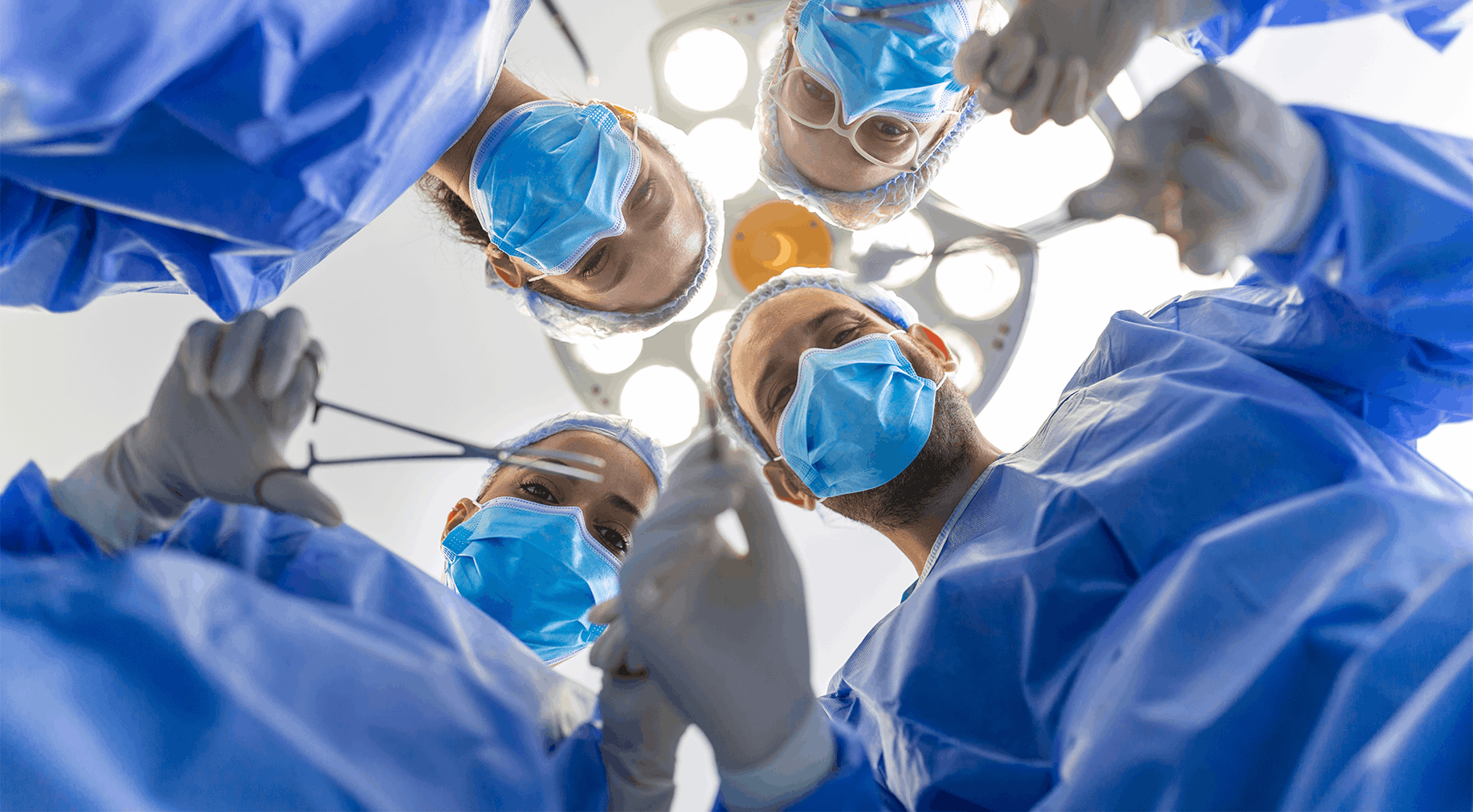
Emergency assessment begins immediately with evaluation of airway, breathing, and circulation. Oxygen saturation is monitored continuously, and supplemental oxygen is administered when indicated. Respiratory rate, effort, and lung sounds are assessed carefully. Simultaneously, heart rate and blood pressure are evaluated to detect cardiovascular instability. In severe cases, airway protection and advanced respiratory support may be required.
The differential diagnosis of acute dyspnea is broad. Respiratory causes include asthma exacerbation, chronic obstructive pulmonary disease (COPD) flare, pneumonia, pulmonary embolism, pneumothorax, or upper airway obstruction. Cardiac causes may include heart failure, arrhythmias, or myocardial ischemia. Metabolic conditions such as diabetic ketoacidosis or severe anemia can also present with breathlessness. Allergic reactions may cause airway swelling and respiratory compromise. Anxiety-induced hyperventilation is considered only after life-threatening causes are excluded.
Diagnostic testing is guided by clinical findings. Chest imaging may identify infection, fluid overload, or lung collapse. Electrocardiography assesses cardiac rhythm and ischemia. Blood tests evaluate oxygenation, infection markers, metabolic abnormalities, and clotting status. Arterial blood gas analysis may be performed in severe respiratory distress to assess ventilation efficiency.
Management focuses on stabilizing oxygenation and addressing the underlying cause. Bronchodilators relieve airway constriction in asthma or COPD. Diuretics may be administered for heart failure. Anticoagulation is initiated in suspected pulmonary embolism. Antibiotics are given for bacterial pneumonia. In severe respiratory failure, non-invasive or invasive ventilatory support may be necessary.
Continuous monitoring is essential because patients with respiratory compromise can deteriorate quickly. Early identification of worsening oxygen levels, fatigue, or altered mental status prompts escalation of care. Coordination with pulmonary, cardiology, or critical care teams ensures comprehensive management.
Timely emergency evaluation of shortness of breath prevents respiratory failure, cardiac arrest, and long-term complications. Structured protocols emphasize rapid stabilization, systematic exclusion of life-threatening causes, and targeted treatment to restore safe breathing and oxygen delivery.
Quick Contact
If you have any questions simply use the following contact details.

Working Hours
-
Out-patient Department
Monday to Saturday 08:00 AM - 09:00 PM
Sunday 10:00 AM - 06:00 PM
-
Emergency Department & Pharmacy
Sunday to Saturday 24x7

 04 406 3000
04 406 3000  04 406 3000
04 406 3000
Quick Links
Legal
Working Hours
-
Out-patient Department
Monday to Saturday | 8 AM to 9 PM
Sunday | 10 AM to 6 PM
Emergency Department & Pharmacy | 24x7
Connect with us!








©2026 IMH. All Rights Reserved. Ministry of Health License No : YP7TYZVC-090326